
Say Goodbye to Hip Pain: Comprehensive Information on Hip Implant Options from Dr. Ahmet Kaplan
Hello, I am Dr. Ahmet Kaplan, a specialist in Orthopedics and Traumatology. For years, I have been helping patients in my clinic who are struggling with musculoskeletal problems that significantly affect their quality of life. Among the foremost of these issues are undoubtedly hip problems. Often arising from wear and tear due to aging or various diseases, hip pain and limited mobility can prevent individuals from performing even the simplest daily tasks. Basic movements like walking, sitting, or climbing stairs can become agonizing. Hip joint damage can also occur in athletes or young individuals who have experienced trauma.
It is precisely at this point that one of modern medicine’s most rewarding solutions comes into play: hip replacement surgery, which involves replacing the damaged hip joint with an artificial implant. When performed on the right patient using the correct technique and the appropriate implant, this surgery quite literally restores freedom of movement to our patients. A life free from pain and a return to active days are no longer just a dream.
So, how does this remarkable solution work? What is a hip prosthesis? When is it necessary? And most importantly, what are the hip implant options? Because there isn’t just one type of hip prosthesis. Every patient, every hip problem is unique, and selecting the most suitable implant based on these individual differences is vitally important for achieving the best outcome.
Let’s explore the answers to these questions together, starting with the fascinating structure of our hip joint. My aim is to convey this topic to you in an understandable, friendly manner, without getting bogged down in technical details, and to address the questions you might have.
Chapter 1: Our Hip Joint: A Marvel of Engineering
Our hip joint is perhaps one of the strongest and most load-bearing joints in our body. The hip joint is formed by the articulation of the deep, cup-shaped socket in the pelvis called the acetabulum and the ball-shaped head of the femur (thigh bone) called the femoral head. You can think of it much like a ball and socket. This ball (femoral head) fits perfectly into the socket (acetabulum).
The surfaces of these bony structures are covered with articular cartilage, a smooth, slippery tissue. The articular cartilage prevents bones from rubbing against each other, facilitates movement, and absorbs loads placed on the joint. The joint capsule and strong ligaments hold this structure together, while the surrounding muscles (hip muscles, thigh muscles) allow us to move and support the joint.
The primary function of the hip joint is to bear our body weight and enable us to perform a wide range of movements such as walking, running, jumping, bending, and sitting. Thanks to this perfect fit and function, we often go about our lives without even noticing its presence. However, when this delicate balance is disrupted, when the joint surfaces are damaged or their congruity is lost, hip pain and loss of function become inevitable.
Chapter 2: Why Does the Hip Hurt? Common Problems and Causes
While hip pain can occur at any stage of life, it is more common, especially after middle age and in older adulthood. There can be numerous underlying causes for this pain. The conditions I most frequently encounter in my clinic that may necessitate hip prosthesis surgery include:
Osteoarthritis: This is by far the most common reason for hip replacement surgery. Also known in medical terms as degenerative joint disease, osteoarthritis is a condition where the articular cartilage wears away, thins, and eventually disappears over time. When the cartilage is lost, bones begin to rub against each other. This friction leads to pain, stiffness, limited mobility, and joint deformity. Osteoarthritis can be a natural consequence of aging, but it can also be accelerated or appear earlier in life by factors such as genetic predisposition, obesity, past joint injuries, congenital joint problems, or overuse. Patients typically experience severe pain during walking, climbing stairs, or getting up after sitting for a long time.
Rheumatoid Arthritis and Other Inflammatory Joint Diseases: Rheumatoid arthritis is an autoimmune disease (related to the immune system) in which the body attacks its own joint linings. This inflammation can progressively destroy the articular cartilage and bone. It can affect many joints in the body, not just the hip. Other inflammatory rheumatic diseases like Ankylosing Spondylitis can also cause significant damage to the hip joint, leading to the need for a prosthesis. In these diseases, pain and stiffness may be pronounced, especially in the mornings or after periods of inactivity.
Avascular Necrosis (AVN) / Osteonecrosis: This condition results from a disruption in the blood supply to the femoral head, causing the bone tissue to die and collapse. Causes of AVN include long-term corticosteroid use, excessive alcohol consumption, smoking, trauma (hip dislocation or fracture), blood disorders like sickle cell anemia, radiation therapy, and some metabolic diseases. The femoral head, deprived of sufficient blood flow, becomes unable to bear the load placed upon it, its shape is distorted, and pain begins. AVN can affect young or middle-aged individuals and is a progressive condition.
Post-Traumatic Conditions: Hip fractures (especially femoral neck fractures and acetabular fractures) or severe hip dislocations can cause permanent joint damage. Disruption of blood supply by the fracture line (risk of AVN), damage to the joint surfaces, or malunion (poor healing) of the fracture can result in severe pain and arthritis development. Femoral neck fractures, particularly common in elderly patients, usually require urgent surgery and often a partial or total hip prosthesis.
Congenital Hip Dislocation (Developmental Dysplasia of the Hip) and Other Congenital Deformities: If the hip joint does not develop properly from birth or is dislocated, the joint surfaces bear weight abnormally, leading to severe arthritis over time. Since the anatomical structure of these patients may be different, prosthesis surgery can be more complex and require special implants.
Any of these conditions can disrupt the normal function of the hip joint, leading to pain, stiffness, difficulty walking, and a decrease in overall quality of life. Initial treatments like pain relievers and physical therapy may provide some relief, but if the joint damage is severe, surgery is the definitive solution.
As Dr. Ahmet Kaplan, I discuss this process thoroughly with each of my patients. The treatment decision is made together, based on the patient’s age, general health status, activity level, pain severity, degree of joint damage, and most importantly, the patient’s expectations. The decision for surgery is generally made when all other methods have been tried and failed, and the patient’s quality of life has significantly deteriorated to an unacceptable level.
Chapter 4: Hip Prosthesis (Implant): Restoring Freedom of Movement
Hip prosthesis, medically known as arthroplasty, is the procedure of removing damaged hip joint surfaces and replacing them with artificial parts (implants). These artificial parts are typically made from special alloyed metals (titanium, cobalt-chromium), high-density polyethylene plastic, or ceramic. These materials are biocompatible (compatible with the body) and resistant to wear.
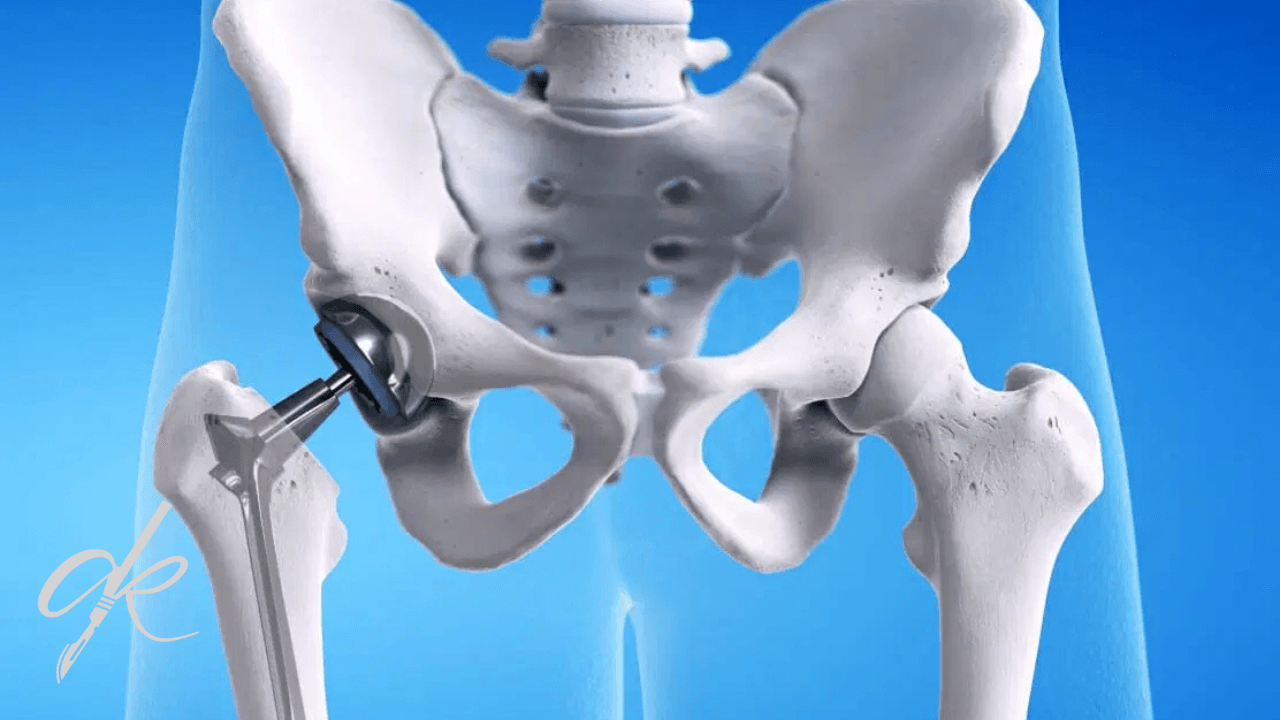
The primary function of a hip prosthesis is to replace the damaged joint surfaces, providing painless and smooth movement. The damaged cartilage and bone in the acetabulum (pelvic bone) are cleaned out, and an artificial socket (acetabular component) is implanted. The femoral head is cut off and replaced with an artificial head (femoral head) attached to a stem inserted into the thigh bone (femoral stem). This new head moves within a special liner inside the artificial socket. This artificial ball-and-socket system, just like a healthy hip joint, offers painless and extensive range of motion.
Modern hip prosthesis surgery dramatically reduces or eliminates patients’ pain, restores their ability to walk, enables them to perform daily activities, and significantly improves their overall quality of life. For many people who have lived with pain for years, this feels like a new lease on life.
Chapter 5: Hip Implant Options: A Multifaceted Decision Process
As I mentioned earlier, there is no single “best” hip prosthesis. The best prosthesis is the one chosen based on the patient’s individual needs, age, activity level, bone quality, and underlying condition. Here are the main types of hip implants and their characteristics:
5.1 Total Hip Arthroplasty (THA):
This is the most commonly performed and well-known type of hip prosthesis. It refers to the surgery where both the socket in the acetabulum and the femoral head are replaced. It is the gold standard treatment for conditions affecting the entire joint, such as severe osteoarthritis, rheumatoid arthritis, and avascular necrosis.
THA consists of three main components:
Femoral Component: This part is inserted into the thigh bone (femur). It consists of a stem inserted into the bone and a ball-shaped head attached to the stem. The stem is usually made of titanium or cobalt-chromium alloy. Two main methods are used to fix the stem to the bone:
- Cemented Prostheses: The stem is fixed inside the bone using a special bone cement (Polymethyl methacrylate – PMMA). It is generally preferred for older patients with poor bone quality or in certain revision (re-operation) situations. The advantage is that it allows immediate weight-bearing.
- Uncemented Prostheses: The surface of the stem is rough or specially coated (like hydroxyapatite) to encourage bone growth onto it. The stem is tightly pressed into the bone, and the bone is expected to grow onto the surface of the prosthesis over time. It is preferred for younger, active patients with good bone quality due to its potential for long-term durability. Bone ingrowth takes several weeks or months.
- Hybrid Prostheses: In this approach, the acetabular socket is usually uncemented, while the femoral stem is cemented. This aims to benefit from the advantages of both methods.
Acetabular Component: This part is placed inside the natural socket in the pelvic bone. It usually consists of a metal outer shell and a liner that fits inside this shell. The outer shell is typically pressed into the bone uncemented or fixed with screws. Rarely, a cemented method may also be used. The liner is the surface within the socket where the head moves, and it can be made of different materials (polyethylene, ceramic, or metal). These materials will be discussed in more detail in the next chapter.
Femoral Head: This is the ball-shaped part attached to the end of the femoral stem. It articulates with the liner inside the acetabular component, allowing joint movement. It is made of ceramic or metal. The size of the head affects joint stability and range of motion. Generally, larger heads provide more stability, but wear risk varies depending on the material.
Advantages of THA: Highly successful in relieving pain, significantly restores range of motion, and with modern implants, its lifespan is typically 20-25 years or more. The vast majority of patients can return to normal or near-normal activity levels.
Disadvantages of THA: It is a major surgery, carries risks such as infection, dislocation, loosening, leg length discrepancy (these will be detailed in the risks section). The recovery process requires patience.
Surgical Approaches: Different surgical approaches (the path through which the incision is made and muscles are accessed) are used for THA surgery. The most common ones are posterolateral (from the back-side), direct lateral (directly from the side), and direct anterior (directly from the front) approaches. Each approach has its own advantages and disadvantages (may differ in terms of muscle damage, recovery speed, and dislocation risk). The most suitable approach is chosen based on the surgeon’s experience and the patient’s anatomy. As Dr. Ahmet Kaplan, I determine the most appropriate surgical technique based on the patient’s condition and the goal of achieving the best results.
5.2 Hemiarthroplasty:
In this method, only the femoral head and neck are cut and removed, and replaced with an artificial component consisting of a femoral stem and head. The acetabulum socket in the pelvic bone is not implanted; the femoral prosthesis head articulates directly with the patient’s own acetabular cartilage.
Hemiarthroplasty is usually preferred for femoral neck fractures in elderly, less active patients with poor bone quality. The shorter surgical time and less bone removal compared to total replacement can reduce surgical stress for these patients.
Advantages of Hemiarthroplasty: Shorter surgical time, less blood loss, no surgical intervention on the acetabulum compared to total replacement. Disadvantages of Hemiarthroplasty: Higher risk of wear and pain in the acetabulum over time due to the prosthesis head rubbing against the patient’s own cartilage. Therefore, it is generally not preferred for younger or active patients due to the higher risk of needing a total replacement in the future. Hemiarthroplasty is typically used to quickly relieve symptoms in situations where the patient’s life expectancy or activity level is low.
5.3 Hip Resurfacing Arthroplasty:
This is a less common type of prosthesis and is generally considered for young, active patients with very good bone quality. In hip resurfacing, the femoral head is not completely cut off; instead, a thin metal cap is placed over the surface of the femoral head and inside the acetabular socket. This means a significant portion of the bone is preserved.
Advantages of Hip Resurfacing: More bone preservation, thought to provide a more natural range of motion and feel, potential for easier revision surgery if needed in the future. Disadvantages/Risks: Risk of metal ion release due to metal-on-metal articulation (this will be detailed in the materials section), risk of femoral neck fracture (especially in women and those with borderline bone quality), the surgical technique is more demanding. The use of hip resurfacing has significantly decreased in recent years due to the risks of metal ion release and is only performed in very specific situations by experienced surgeons on carefully selected patients.
5.4 Dual Mobility Implants:
This prosthesis design was developed specifically for patients with a high risk of hip dislocation. In traditional prostheses, the metal or ceramic head moves within a polyethylene-lined metal socket. In dual mobility implants, a smaller head (usually ceramic) is placed within a larger, thick-walled polyethylene “second head.” This polyethylene second head then moves freely within the metal shell. Thus, the prosthesis has two points of articulation: the movement of the head within the polyethylene, and the movement of the polyethylene within the shell.
Advantage of Dual Mobility Implants: The range of motion required for the prosthesis to dislocate from its socket is much greater, dramatically reducing the risk of dislocation. It can be preferred especially in patients who have previously experienced hip dislocation, those with poor muscle control, or in revision surgeries. Disadvantage of Dual Mobility Implants: It is a more complex structure, carrying specific rare risks such as “intraprosthetic dislocation,” where the polyethylene second head comes out of the metal shell. The potential for wear is theoretically slightly different due to having multiple articulating surfaces.
These prosthesis types are the main options evaluated by the surgeon based on the patient’s condition. However, the quality and compatibility of the materials used in the implant are just as important as the type of prosthesis for its success.
Chapter 6: Prosthesis Materials: Friction, Wear, and Lifespan
One of the most critical factors determining the lifespan, durability, and biocompatibility of hip prostheses is the materials used for the articulating surfaces (head and liner/socket). The friction between these materials and the wear that occurs over time directly affect the lifespan of the prosthesis. Here are the main material combinations:
6.1 Metal-on-Polyethylene Articulation:
This is the traditional and most commonly used combination, with the longest follow-up results in hip prosthesis surgery. Typically, a metal head made of cobalt-chromium alloy articulates within a socket liner made of high-density polyethylene plastic.
- Conventional Polyethylene: Used as the standard for many years. However, over time, very small particles (wear debris) flake off the polyethylene surface due to friction with the metal head. These particles can cause an inflammatory reaction in the body, leading to bone resorption (osteolysis) around the prosthesis and ultimately causing the prosthesis to loosen. This was the most common reason requiring revision surgery, often after 10-15 years.
- Highly Cross-linked Polyethylene (XLPE): This is a new generation of polyethylene developed in the last 20 years that has brought about a revolution in hip prosthesis surgery. Through a special process (cross-linking followed by melting/annealing), the molecular structure of polyethylene is made more durable. XLPE reduces the formation of wear particles by up to 90% compared to conventional polyethylene. This significantly lowers the risk of osteolysis and loosening, extending the lifespan of the prosthesis.
Advantages (Especially with XLPE): Proven long-term reliability, low wear rate (XLPE), cost-effectiveness (compared to ceramic-on-ceramic). Disadvantages: Risk of wear with conventional polyethylene, rare risk of liner fracture (very rare).
6.2 Ceramic-on-Ceramic Articulation:
In this combination, both articulating surfaces are made of ceramic (usually alumina or zirconia ceramic).
Advantages: Ceramic has the lowest known wear rate. Therefore, it has a very high potential to extend the lifespan of the prosthesis, especially in young, active patients with a long life expectancy. The risk of osteolysis is very low. Disadvantages: Ceramic is brittle. Rarely, there is a risk of fracture, especially when exposed to high impact or sudden loads (although current ceramics are more durable, the risk is not completely zero). Another potential issue is the “squeaking” sound that can occur, particularly in the initial period of use or if the surfaces are not adequately lubricated. This sound can be bothersome but usually decreases or disappears over time. It is a high-cost option.
6.3 Ceramic-on-Polyethylene Articulation:
This is one of the most popular and widely used combinations today. The femoral head is made of ceramic (for its low wear property), and this head articulates within a highly cross-linked polyethylene (XLPE) liner.
Advantages: Combines the low wear property of ceramic with the reduced wear of XLPE. It offers a lower wear rate and risk of osteolysis compared to metal-on-polyethylene. It has less brittleness risk and a lower squeaking potential compared to ceramic-on-ceramic. The cost is usually between metal-on-polyethylene and ceramic-on-ceramic. It offers an ideal balance for many patients. Disadvantage: Although not as low as ceramic-on-ceramic, XLPE still has some potential for wear (though better than metal-on-polyethylene). The rare risk of ceramic head fracture persists.
6.4 Metal-on-Metal Articulation:
In this combination, both the femoral head and the acetabular socket are made of metal (usually cobalt-chromium alloy). In the past, it became popular, especially for hip resurfacing and some total hip models, promising high durability and low wear.
Advantages: High durability, theoretically very low wear rate (however, the practical outcome was different). Disadvantages: The most significant disadvantage and the reason its use is very limited today is the release of metal ions (cobalt and chromium) into the bloodstream due to friction. These metal ions can accumulate in the body and cause various problems:
- Allergic Reactions: Some patients may develop a metal allergy.
- Local Tissue Reactions: Risk of developing “pseudotumors,” which are inflammatory reactions and damage to muscle and nerve tissue around the prosthesis, sometimes appearing as a mass. This can cause pain, swelling, and loosening of the prosthesis.
- Systemic Effects: There are concerns about the potential long-term effects of high levels of metal ions on other organs such as the heart, kidneys, and nervous system.
Due to these serious risks, many metal-on-metal prosthesis models have been recalled, and their use has dramatically decreased worldwide. Today, metal-on-metal prostheses can only be considered in very rare and specific cases, for selected patients who are fully informed about all risks and are closely monitored. As Dr. Ahmet Kaplan, I prefer not to use metal-on-metal prostheses routinely due to these potential risks.
The choice of prosthesis material is an important decision influenced by many factors including the surgeon’s experience, the patient’s general health, age, activity expectations, and bone structure, and it must be discussed in detail with the patient.
Chapter 7: Choosing the Right Implant: A Personalized Approach
Hip prosthesis surgery is a major step that can fundamentally change a patient’s quality of life. To take this step as successfully as possible, selecting the most suitable implant is of great importance. For me, every patient is different, every hip problem is different. Therefore, the choice of prosthesis is never made with a standard approach; it is entirely personalized.
Let me share what I consider as an Orthopedic Specialist when choosing the right implant:
- Patient’s Age: The expectations and load placed on the prosthesis by a young and active patient are different from those of an elderly and less active patient. For younger patients, more durable and long-lasting options like ceramic-on-ceramic or ceramic-on-XLPE articulations, or bone-preserving options like hip resurfacing (in very selected cases), might be considered. For elderly patients, options with proven reliability like metal-on-XLPE or cemented prostheses might be more suitable.
- Activity Level and Lifestyle: The prosthesis choice will differ between someone leading a sedentary life and someone who regularly participates in sports or has a job requiring heavy physical activity. More active individuals require materials more resistant to wear.
- Bone Quality (Bone Density): In patients with weakened bones due to osteoporosis, cemented or specially designed uncemented prostheses may be needed for good fixation to the bone. In patients with good bone quality, uncemented prostheses can integrate with the bone more easily.
- Body Weight: In overweight patients, the load on the prosthetic joint is greater. In such cases, more durable articulation materials and strong fixation methods may be preferred.
- Anatomical Structure and Deformities: If there are anatomical differences such as congenital hip dislocation or deformities due to previous surgeries, specially designed (custom-made) or revision prostheses might be necessary instead of standard ones.
- Underlying Health Conditions: Systemic diseases like diabetes and rheumatoid arthritis can affect bone quality, infection risk, and the healing process. These factors also play a role in prosthesis selection.
- History of Metal Allergy: It is important to avoid metal-containing articulations (metal-on-polyethylene, metal-on-metal, ceramic-on-metal) in patients with allergies to metals like cobalt or chromium. In such cases, prostheses predominantly made of titanium and ceramic are evaluated.
- Reason for Surgery: Is it arthritis, fracture, AVN, or another reason? This is a primary determinant of the prosthesis type (total vs. partial).
- Patient’s Expectations: What level of activity does the patient expect after surgery? What sports do they want to play? These expectations shape the surgeon’s recommendations regarding the prosthesis and surgical technique.
After evaluating all these factors, my team and I determine the most suitable prosthesis type and material. I share this process openly and transparently with my patient, explaining the advantages, disadvantages, and potential risks of the prosthesis options in detail. The final decision is made jointly with the patient’s informed participation. Remember, the most successful outcomes are achieved through open communication based on trust between the surgeon and the patient.
Chapter 8: The Hip Replacement Surgery: How Does the Process Work?
Hip replacement surgery is a major surgery, although frequently performed in Orthopedics and Traumatology practice. The process typically involves the following steps:
- Pre-operative Preparation: Various tests such as blood tests, ECG, chest X-ray are performed to evaluate your general health status. You will be evaluated by an anesthesiologist. Your current medications will be reviewed, and some may need to be stopped before surgery. Pre-operative skin preparation (showering, special soaps) may be done to reduce the risk of infection.
- Anesthesia: The surgery is generally performed under general anesthesia (being completely asleep) or spinal/epidural anesthesia (numbing the lower body). Your anesthesiologist will determine the safest and most suitable anesthesia method for you.
- Surgical Procedure: After the surgical team is ready and anesthesia is administered, an incision is made in the skin to access the hip joint (the location and size of the incision vary depending on the surgical approach used). The surgeon approaches the hip joint by working through or temporarily separating muscles. The damaged femoral head is cut off and removed. The damaged cartilage in the acetabulum socket in the pelvic bone is cleaned out and prepared for the placement of the prosthetic socket. The prosthesis components (acetabular socket, femoral stem, head) are inserted into the bone and fixed (using cemented or uncemented technique). The stability and range of motion of the implanted prosthesis are checked. A thin tube called a drain may be placed to drain excess blood from the surgical area (not always necessary). The incision site is closed with stitches or staples and bandaged.
- Surgery Duration: Hip replacement surgery usually takes 1 to 2 hours, but it can vary depending on the patient’s condition and the complexity of the surgery.
- Post-operative Monitoring: After surgery, you may be taken to the recovery room or intensive care unit for close monitoring. Pain control, monitoring for bleeding, and assessment of your general health status are performed.
This process may seem stressful to the patient, but thanks to modern anesthesia techniques and surgical methods, your comfort is ensured throughout the surgery, and post-operative pain management is effectively provided.
Chapter 9: The Post-Surgery Period: The Journey to Recovery
The success of hip prosthesis surgery depends as much, or perhaps even more, on the post-operative period, especially rehabilitation, as on the surgery itself. Achieving your full potential with your new hip requires patience, discipline, and adherence to physical therapy.
- Hospital Stay: Most patients stay in the hospital for 3 to 5 days after surgery. During this time, your pain control will be managed, measures will be taken to reduce the risks associated with bed rest (such as blood clots), and you will start taking your first steps with a physical therapist.
- Pain Management: Post-operative pain is expected, but it is managed effectively with various methods, including intravenous, oral, or spinal medications. Keeping your pain under control is crucial for early mobilization and participation in physical therapy.
- Early Mobilization: One of the most important steps after surgery is getting out of bed and starting to walk with a physical therapist as soon as possible (usually a few hours after surgery or the next day). Early mobilization increases blood circulation, reduces the risk of blood clots, works the muscles, and speeds up the healing process.
- Physical Therapy and Rehabilitation: This is the cornerstone of the recovery process. Physical therapy, which begins in the hospital, continues at outpatient rehabilitation centers or at home after discharge. Your physical therapy program will include:
- Strengthening Exercises: Exercises to strengthen the muscles around the hip and leg (especially the hip abductors – muscles that move the leg sideways). Strong muscles help stabilize the prosthesis and make walking easier.
- Range of Motion Exercises: Exercises aimed at regaining and maintaining the range of motion in the hip joint within the limits allowed by your prosthesis.
- Gait Training: Re-learning the correct walking pattern. Initially, a walker or crutches are used, and support is gradually reduced until you can walk without assistance.
- Balance and Coordination Exercises: Learning to move safely.
- Use of Assistive Devices: Information on using assistive devices that make daily life easier, such as walkers, crutches, special toilet seat risers, sock aids, etc.
- Precautions and Restrictions: In the first few weeks after surgery, it is important to avoid certain movements depending on the surgical approach and prosthesis type. These “precautions” usually include positions that prevent the prosthesis from dislocating, such as avoiding bending the hip beyond a certain angle (usually 90 degrees), not crossing your legs, and avoiding excessive inward or outward rotation of the hip. Your surgeon and physical therapist will give you detailed information on this. Following these rules is vital for reducing the risk of dislocation.
- Full Recovery and Return to Normal Activities: Full recovery and return to normal daily activities (walking, light sports, household chores) generally takes 3 to 6 months. However, this duration can vary from person to person, depending on general health, success of rehabilitation, and the scope of the surgery. Return to high-impact sports (running, jumping, contact sports) is generally not recommended, as these activities can accelerate prosthesis wear or lead to loosening. Low-impact sports like swimming, cycling, walking, and golf are usually safe.
Remember, recovery is a marathon, not a sprint. Be patient, listen to your physical therapist, exercise regularly, and take good care of your body.
Chapter 10: Potential Risks and Complications
As with any surgical procedure, hip replacement surgery carries potential risks and complications. While these risks are low with modern medicine and surgical techniques, it is important for you as a patient to be aware of them. As Dr. Ahmet Kaplan, I discuss these risks in detail with each of my patients before surgery and answer any questions they may have.
The main risks include:
- Infection: This is one of the most serious complications in prosthesis surgery. If an infection develops in the tissues around the prosthesis, additional surgeries and long-term antibiotic treatment may be necessary, and in some cases, the prosthesis may even need to be removed. Measures are taken before, during, and after surgery to reduce the risk of infection (antibiotic use, sterile operating room conditions, hygiene rules).
- Dislocation: This occurs when the prosthesis head comes out of its socket. It usually happens in the first few months after surgery if specific movement restrictions are not followed. Dislocation may require manipulation or surgery to put the prosthesis back in place. The surgical technique, prosthesis type (dual mobility implants have a lower dislocation risk), and the patient’s adherence to movement restrictions reduce the risk of dislocation.
- Blood Clots (Deep Vein Thrombosis – DVT): There is a risk of blood clots forming in the leg veins. These clots can break off and travel to the lungs, leading to a life-threatening condition called Pulmonary Embolism. To reduce this risk, blood-thinning medications are started before or immediately after surgery, elastic stockings are worn, and early mobilization is encouraged.
- Leg Length Discrepancy: There may be a slight difference in leg length after surgery. The surgeon takes care to equalize leg length during surgery, but sometimes perfect equalization may not be possible, or a slight difference may be necessary for prosthesis stability. Generally, this difference is less than 1-2 cm and becomes tolerable over time or with special shoe inserts.
- Nerve Injury: Nerves around the hip can be stretched or, rarely, damaged during surgery. This can lead to numbness, tingling, or muscle weakness in the leg. It is usually temporary, but rarely can be permanent.
- Prosthesis Loosening or Wear: After many years, the prosthesis may separate from the bone (loosening) or the articulating surfaces may wear out, leading to pain and instability. This requires revision (re-do) surgery. The choice of prosthesis material and surgical technique affects these risks.
- Periprosthetic Fracture: Rarely, a fracture can occur in the bone around the prosthesis during surgery or as a result of trauma like a fall after surgery.
- General Risks of Surgery: General risks associated with any major surgery, such as reactions to anesthesia, heart attack, or stroke, are also present at very low rates.
It is important that you are fully informed about all these risks. However, remember that with modern surgical techniques, sterilization protocols, measures to prevent blood clots, and early rehabilitation, the incidence of these complications is quite low. Your surgeon’s experience and strict adherence to post-operative instructions will help minimize these risks.
Chapter 11: Implant Lifespan and Long-Term Success
One of the most frequently asked questions is: “How long does a hip implant last?” Modern hip prostheses are much more durable than older ones. Current data shows that, depending on the type of prosthesis, materials, surgical technique, and most importantly, individual patient factors, 80-90% of total hip prostheses function without problems for 15-20 years, and some even for 25 years or more. Particularly, the low wear rates of highly cross-linked polyethylene and ceramic-on-ceramic articulations have the potential to extend prosthesis lifespan.
Factors affecting the lifespan of the prosthesis include:
- Patient’s Age and Activity Level: Younger and very active patients may put more load on the prosthesis and experience more wear, potentially shortening its lifespan.
- Body Weight: Excess weight increases stress on the prosthesis.
- Bone Quality: Weak bone can increase the risk of prosthesis loosening.
- Type of Prosthesis and Materials Used: Materials more resistant to wear (ceramic, XLPE) and prosthesis designs that provide stable fixation tend to have a longer lifespan.
- Surgical Technique: A prosthesis placed with the correct technique by an experienced surgeon is more likely to last longer.
- Post-operative Care: Adherence to rehabilitation, avoiding risky movements, and maintaining an ideal body weight help extend the lifespan of the prosthesis.
Revision Surgery: The surgery performed to replace a primary prosthesis that has reached the end of its lifespan, loosened, worn out, become infected, or repeatedly dislocated is called revision hip replacement surgery. Revision surgeries are generally more complex than primary surgeries, may involve more bone loss, and the recovery period can be longer. Therefore, it is very important to extend the lifespan of the primary prosthesis as much as possible.
Long-Term Success: The success of hip prosthesis surgery is measured not only by how long the prosthesis remains in place, but also by how much the patient’s pain is reduced, how much their functional level is increased, and how much their overall quality of life is improved. In most patients I see in my clinic, after proper implant selection and successful surgery, years of pain and limitation are replaced by painless freedom of movement and an active life. This is the greatest source of satisfaction for an orthopedic surgeon.
Follow-up Appointments: Regular doctor check-ups after hip prosthesis surgery are very important. You will be checked several times in the first year, and then usually annually. X-rays taken during these check-ups monitor the position of the prosthesis, its relationship with the bone, and signs of wear. Potential problems can be detected early, and necessary measures can be taken.
Chapter 12: Regaining Hip Health with Dr. Ahmet Kaplan: The Consultation Process
If you are experiencing hip pain, if your daily life is limited by this pain, and if previous treatments you have tried have not been sufficient, it’s time to consult an orthopedic and traumatology specialist.
When you come to my clinic, I will first listen to you. I will learn in detail when your pain started, where it is felt, what movements increase or decrease it, and how it affects your daily life. Then, I will perform a thorough physical examination to evaluate the range of motion of your hip joint, muscle strength, posture, and gait.
One of the most basic tools for diagnosis is the X-ray. X-rays of the hip joint taken while standing and in a side view allow me to see the degree of cartilage loss, changes in the bone, the extent of arthritis, and possible deformities in the joint. If necessary, I may request a Computed Tomography (CT) scan for more detailed evaluation of bone structure or Magnetic Resonance Imaging (MRI) to evaluate soft tissues and blood circulation.
Based on all this information, I will make a definitive diagnosis of your hip problem. We will evaluate treatment options together. If surgery is necessary, I will explain the reasons why it is needed, which type of prosthesis would be most suitable for you, how the surgery will be performed, the recovery process, and potential risks, all with complete transparency. Answering all your questions is my priority. The treatment decision is a joint decision made by the patient and the physician together, after discussing all alternatives and risks.
In my philosophy, surgery is just the beginning. The key to success is accurate diagnosis, correct implant selection, flawless surgical technique, and most importantly, effective post-operative rehabilitation. In my clinic, I aim to be by your side throughout every stage of this process.
Hip pain should not be a condition that forces you to postpone your life. Thanks to advancements in modern orthopedics and prosthesis technology, it is now possible to successfully replace a worn or damaged hip joint and offer our patients a life free from pain and a return to activity.
Hip implant options are diverse, and each offers advantages for specific patients and situations. Various types such as total hip replacement, partial hip replacement, hip resurfacing, or dual mobility implants, and different material combinations like metal-on-polyethylene, ceramic-on-ceramic, and ceramic-on-polyethylene are available. Making the most suitable choice requires a careful evaluation of many factors including the patient’s age, activity level, bone quality, general health status, and expectations. This is only possible after a detailed evaluation and discussion with an experienced Orthopedics and Traumatology Specialist.
As Dr. Ahmet Kaplan, I aim to provide a personalized approach to each of my patients in my clinic, creating the most suitable treatment plan for their needs. Hip prosthesis surgery, when performed by skilled hands and with proper planning, can significantly improve your quality of life, relieve you from years of suffering from pain, and restore your freedom of movement.
If you are experiencing hip pain and your quality of life is negatively affected, do not delay. Consult an orthopedic specialist to learn about your personalized treatment options. Remember, every step you take towards better health opens the doors to a higher quality of life.
I wish you healthy, pain-free, and active days.
Dr. Ahmet Kaplan



